Free Oregon 53 05A Form
Oregon PDF Docs
Free Oregon 53 05A Form
The Oregon 53 05A form, formally known as the Certificate of Immunization Status, plays a crucial role in ensuring that children attending schools, preschools, child care facilities, or home daycares in Oregon are properly immunized against preventable diseases. This document not only serves as proof of immunization but also facilitates the collection of essential information on behalf of the Oregon Health Authority's Immunization Program. Parents or guardians must complete this form, providing details such as the child's full name, birthdate, and contact information, alongside a comprehensive list of vaccines received. The form requires the dates of each immunization to be recorded in the order they were administered, ensuring clarity and accuracy in tracking a child's vaccination history. Additionally, the Oregon 53 05A form accommodates exemptions, allowing parents to decline specific vaccines for medical or nonmedical reasons, provided that the appropriate documentation is submitted. By filling out this form, parents not only comply with state law but also contribute to the broader public health initiative aimed at preventing outbreaks of vaccine-preventable diseases.
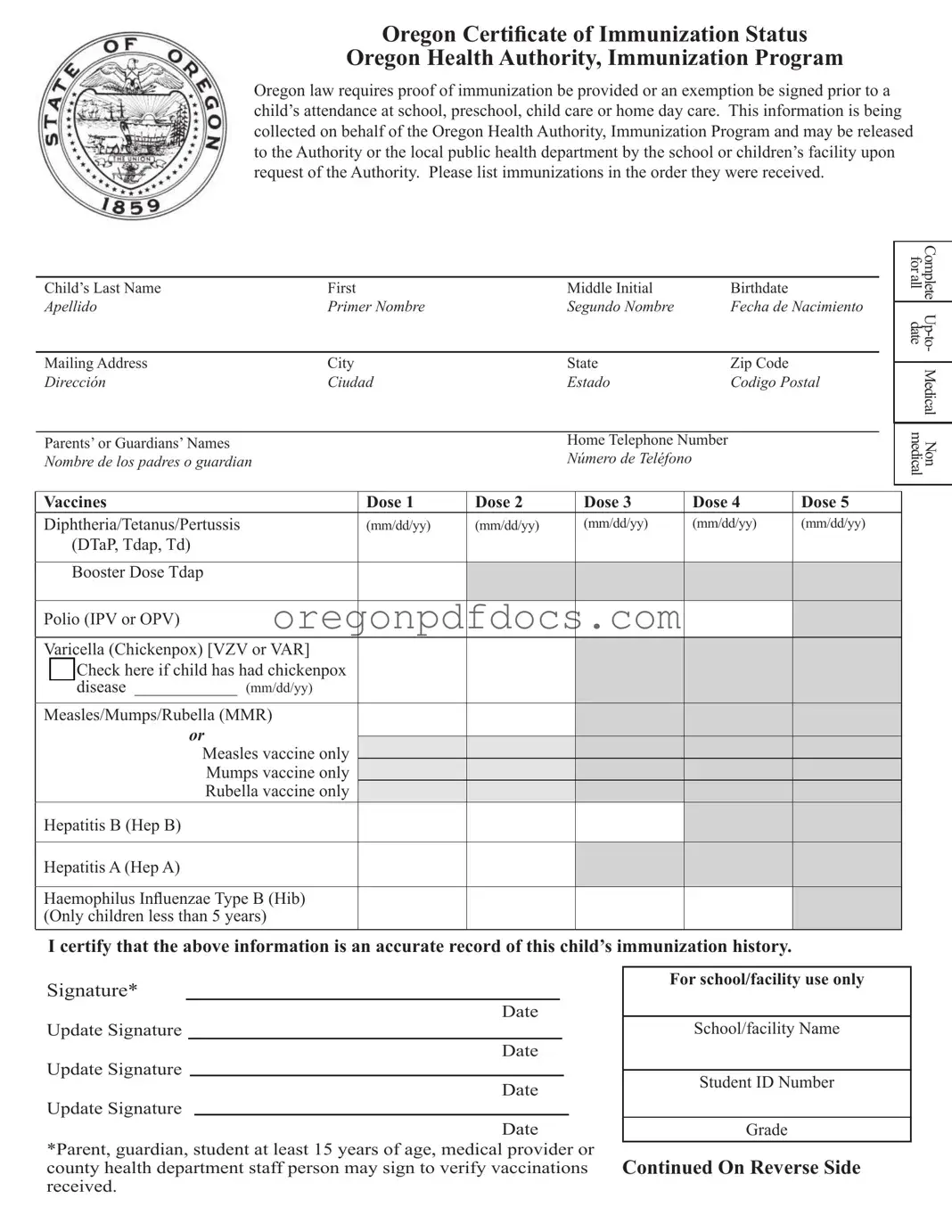
Oregon Certi! cate of Immunization Status
Oregon Health Authority, Immunization Program
Oregon law requires proof of immunization be provided or an exemption be signed prior to a child’s attendance at school, preschool, child care or home day care. This information is being collected on behalf of the Oregon Health Authority, Immunization Program and may be released to the Authority or the local public health department by the school or children’s facility upon request of the Authority. Please list immunizations in the order they were received.
Child’s Last Name |
First |
|
Middle Initial |
Birthdate |
|
|
||
Apellido |
Primer Nombre |
|
Segundo Nombre |
Fecha de Nacimiento |
|
|||
|
|
|
|
|
|
|
|
|
Mailing Address |
City |
|
State |
Zip Code |
|
|
||
Dirección |
Ciudad |
|
Estado |
Codigo Postal |
|
|||
|
|
|
|
|
|
|
|
|
Parents’ or Guardians’ Names |
|
|
Home Telephone Number |
|
|
|||
Nombre de los padres o guardian |
|
|
Número de Teléfono |
|
|
|
||
|
|
|
|
|
|
|
|
|
Vaccines |
Dose 1 |
Dose 2 |
Dose 3 |
Dose 4 |
Dose 5 |
|
||
Diphtheria/Tetanus/Pertussis |
(mm/dd/yy) |
(mm/dd/yy) |
(mm/dd/yy) |
(mm/dd/yy) |
(mm/dd/yy) |
|
||
|
(DTaP, Tdap, Td) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Booster Dose Tdap |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Polio (IPV or OPV) |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
Varicella (Chickenpox) [VZV or VAR] |
|
|
|
|
|
|
||
|
o |
Check here if child has had chickenpox |
|
|
|
|
|
|
|
|
disease ____________ (mm/dd/yy) |
|
|
|
|
|
|
Measles/Mumps/Rubella (MMR)
or
Measles vaccine only
Mumps vaccine only
Rubella vaccine only
Hepatitis B (Hep B)
Hepatitis A (Hep A)
Haemophilus In! uenzae Type B (Hib) (Only children less than 5 years)
I certify that the above information is an accurate record of this child’s immunization history.
for all |
Complete |
|
Medical |
medical |
Non |
Signature*
Date
Update Signature
Date
Update Signature
Date
Update Signature
Date
*Parent, guardian, student at least 15 years of age, medical provider or county health department staff person may sign to verify vaccinations received.
For school/facility use only
School/facility Name
Student ID Number
Grade
Continued On Reverse Side
Oregon Certificate of Immunization Status, Page 2
Oregon Health Authority, Immunization Program
Child's Last Name |
First |
Middle Initial |
Birthdate |
Apellido |
Primer Nombre |
Segundo Nombre |
Fecha de Nacimiento |
� |
Recommended Vaccines |
|
Pneumococcal (PCV) |
||
= |
||
...� |
(Only in children less than 5 years) |
|
� |
|
|
"CS |
Meningococcal (MCV4, MPSV4) |
|
|
||
� |
Human Papilloma Virus (HPV) |
|
"CS |
||
e |
(9 years or older) |
|
= |
||
� |
|
|
e |
Influenza (Flu) |
�
�Other Vaccine
�Please specify:
Other Vaccine Please specify:
For medical exemptions:
Please submit a letter signed by a licensed physician stating:
•Child's name
•Birth date
•Medical condition that contraindicates vaccine
•List of vaccines contraindicated
•Approximate time until condition resolves, if applicable
•Physician's signature and date
•Physician's contact information, including
phone number
For Immunity Documentation (history ofdisease or positive titer): Please submit a letter signed by a licensed physician stating:
•Child's name and birth date
•Diagnosis or lab report
•Physician's signature and date
Dose 1 |
Dose2 |
Dose3 |
Dose4 |
Doses |
Nonmedical Exemption:
I have received information regarding the benefits and risks of immunizations. I understand that my child may be excluded from school or child care attendance ifthere is a case ofdisease that could be prevented by vaccine. I have attached the required document from (check one):

 A health care practitioner
A health care practitioner

 The vaccine educational module approved by the Oregon Health Authority
The vaccine educational module approved by the Oregon Health Authority
I understand that I may decline one or more vaccinations for my child and request that my |
||||
child be exempted from the following required immunizations (check all that apply): |
||||
|
|
Diphtheria/ Tetanus/Pertussis |
|
Hepatitis B |
|
|
|
||
|
|
Polio |
|
Hepatitis A |
|
|
|
||
|
|
Varicella |
|
Hib |
|
|
Measles/Mumps/Rubella |
|
Date |
Signature of Parent or Guardian |
|
|||
Optional:
ORS 433.267 states that this document may include the reason for declining the immunization. Immunization is being declined because of:
Religious belief |
|
Philosophical belief |
|
Other |
I certify that the above information is an accurate record of this child's immunization history and exemption status.
Signature
Date
Update Signature
Update Signature
Update Signature
Date
Date
Date |
Instructions for completing the
Certificate of Immunization Status
Contact information:
Complete information for your child including full name, birthdate, current mailing address, parentsÕ or guardiansÕ names and home telephone number. This information will be used to contact you if there are questions about your childÕs immunization history.
Required vaccines (Front):
Fill in the month/day/year that your child received each dose of vaccine. Doses must be listed in the order received. The shaded boxes on the form indicate doses that are not routinely given, however if your child received them, please write the date in the shaded box. Check with your childÕs school or daycare to find out which vaccines are required for your childÕs age or grade.
Recommended vaccines (Back):
These doses are not required by law, however these vaccines are recommended and most children receive them. Fill in the month/day/year that your child received each dose of vaccine. Doses should be listed in the order received. The shaded boxes on the form indicate doses that are not routinely given, however if your child received them, please write the date in the shaded box.
Signature:
The parent or guardian signature is a sworn statement that the childÕs record is accurate. The signature of a physician or local health department is not required but it is acceptable. Every time
you add on to your child’s information you need to resign the form.
REMEMBER TO COMPLETE BOTH SIDES OF FORM
Exemptions:
Oregon allows medical and nonmedical exemptions.
For a nonmedical exemption, check the appropriate box and submit one of the following required documents:
1.A certificate signed by a health care practitioner verifying discussion of the benefits and risks of immunization, or
2.A certificate of completion of the vaccine educational module about the benefits and risks of
immunization.
Indicate which vaccines you are exempting your child from by checking the boxes. Sign and date on the indicated line.
For a medical exemption or proof of immunity, submit a letter from your childÕs physician to the school or child care.
Instrucciones para llenar el
Certificado de Estado de Vacunación
DŽ la siguiente
Vacunas requeridas (adelante):
Escriba el
Vacunas recomendadas (atr‡s):
Estas dosis no son obligatorias por ley, pero son recomendadas y la mayor’a de los
Firma:
La firma del padre, madre o tutor es una
volver a firmar el formulario.
RECUERDE LLENAR AMBOS LADOS DEL FORMULARIO
Excepciones:
Oregon permite excepciones mŽdicas y no mŽdicas.
Para una
1.Un certificado firmado por un proveedor de
2.Un certificado de
riesgos de la
Indique para cu‡les vacunas quiere que su hijo(a) sea exento(a) al marcar las casillas. Firme y feche la l’nea indicada.
Para una
Oregon Small Claims Court Forms - The form serves as a necessary notice that initiates the legal process for small claims.
In order to facilitate a seamless vehicle transaction in California, it is important for both buyers and sellers to familiarize themselves with the California Vehicle Purchase Agreement form, which can be obtained from legalpdf.org. This legally binding document not only specifies the terms of the sale but also serves as a record of essential details, including the sale price and any warranties provided. Properly completing this form can help avoid ambiguities and ensure that both parties are protected throughout the transaction.
Oregon Income Tax Form - The form outlines the specific legal contexts in which it can be applied, such as marriage or registered domestic partnerships.
| Fact Name | Details |
|---|---|
| Form Purpose | The Oregon 53 05A form serves to document a child's immunization status for school or childcare attendance. |
| Governing Law | Oregon law mandates proof of immunization or a signed exemption prior to a child's attendance at school or childcare facilities. |
| Required Information | Parents must provide the child's full name, birthdate, mailing address, and parents’ or guardians’ names and phone numbers. |
| Immunization Records | Vaccination dates must be listed in the order received, including required and recommended vaccines. |
| Exemption Types | Oregon allows for both medical and nonmedical exemptions from vaccinations. |
| Signature Requirement | A parent, guardian, or eligible individual must sign the form to verify the accuracy of the immunization record. |
| Submission Guidelines | For medical exemptions, a physician's letter detailing the child's medical condition must be submitted along with the form. |
The Oregon 53 05A form, known as the Certificate of Immunization Status, is essential for documenting a child's immunization history before attending school or childcare. Alongside this form, several other documents may be required to ensure compliance with state immunization laws. Below is a list of related forms and documents that are commonly used in conjunction with the Oregon 53 05A form.
Understanding these documents and their purposes can help parents navigate the immunization requirements in Oregon effectively. Having the necessary paperwork ready will facilitate a smoother enrollment process for children entering school or childcare settings.