Free Oregon Registry Enrollment Form
Oregon PDF Docs
Free Oregon Registry Enrollment Form
The Oregon Registry Enrollment form is an essential tool for individuals working in childhood care and education, offering a streamlined way to track professional development and meet licensing requirements. This online enrollment process begins by collecting vital personal information, such as your name, date of birth, and contact details, ensuring that your records are accurately maintained. Additionally, the form includes optional sections that gather demographic information, allowing the Child Care Division to assess inclusivity within the workforce. As you fill out the form, you will also provide details about your position, education level, and the type of facility where you work or volunteer. This comprehensive approach not only helps in organizing your professional journey but also supports the broader goal of improving child care services across Oregon. Finally, by signing the form, you authorize the sharing of your training and education records with relevant agencies, ensuring that your information remains confidential yet accessible to those who need it for your professional development.
Child Care Provider Application: This document collects personal and professional information from individuals seeking to become licensed child care providers. Similar to the Oregon Registry Enrollment form, it includes sections for individual information, employment history, and training qualifications.
Background Check Authorization Form: This form is used to authorize a background check for individuals working with children. Like the Oregon Registry Enrollment form, it requires personal identification details and consent for information sharing.
Professional Development Plan: This document outlines an individual's goals for professional growth in the field of childhood education. It mirrors the Oregon Registry Enrollment form by tracking educational background and training needs.
Child Care Licensing Application: This application is necessary for obtaining a child care license. It parallels the Oregon Registry Enrollment form in that it gathers detailed information about the applicant's qualifications and the facility where they intend to work.
Employee Information Form: Used by employers to collect data on new hires, this form includes sections for personal information, job title, and emergency contacts, similar to the Oregon Registry Enrollment form's emphasis on individual details.
Volunteer Registration Form: This document is utilized by organizations to register volunteers. It shares similarities with the Oregon Registry Enrollment form, particularly in gathering personal information and background related to the volunteer's role.
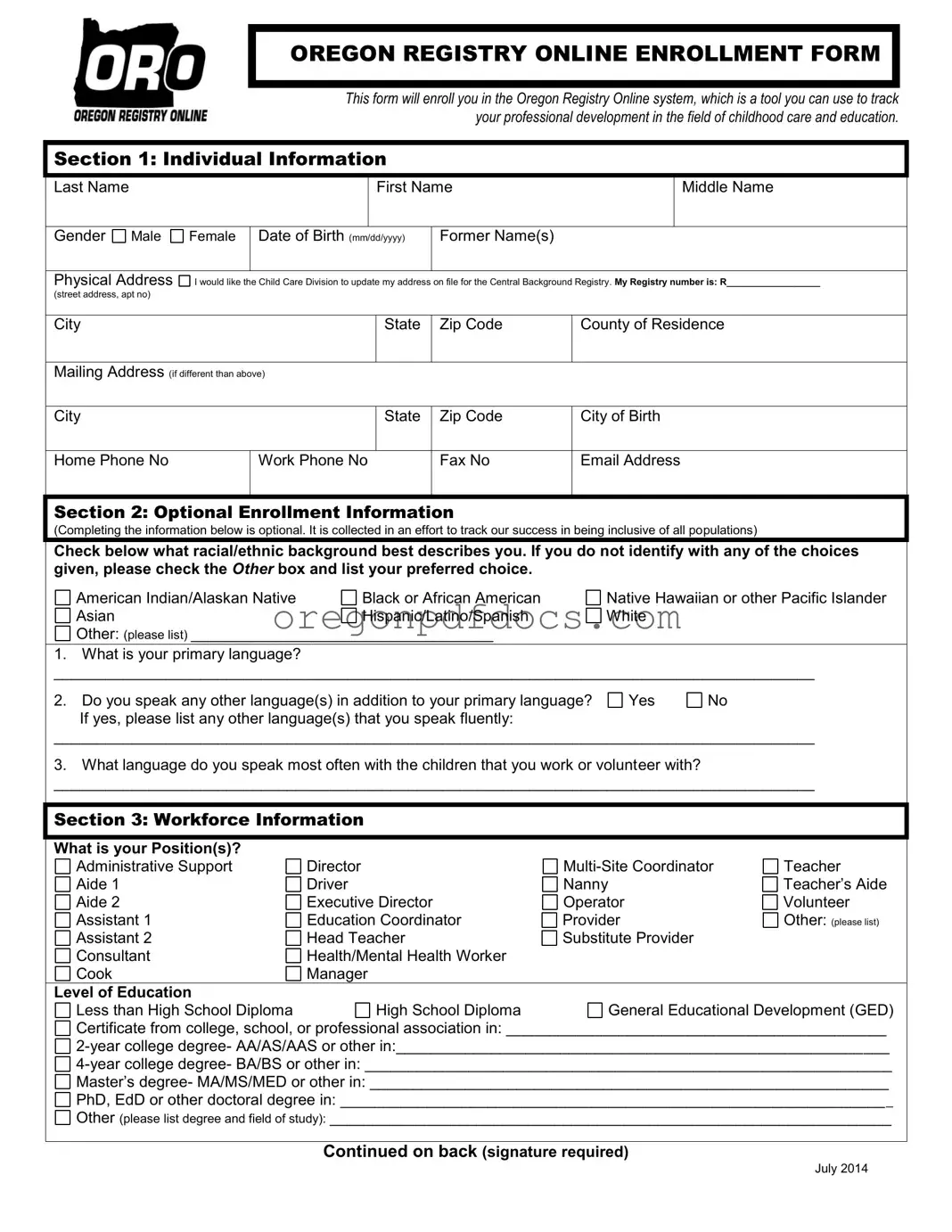
OREGON REGISTRY ONLINE ENROLLMENT FORM
This form will enroll you in the Oregon Registry Online system, which is a tool you can use to track your professional development in the field of childhood care and education.
Section 1: Individual Information
|
Last Name |
|
|
|
First Name |
|
Middle Name |
|
|
|
|
|
|
|
|
|
|
|
Gender Male |
Female |
Date of Birth (mm/dd/yyyy) |
Former Name(s) |
|
|
||
|
|
|
|
|
|
|
||
|
Physical Address |
I would like the Child Care Division to update my address on file for the Central Background Registry. My Registry number is: R__________________ |
||||||
|
(street address, apt no) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
Zip Code |
County of Residence |
|
|
|
|
|
|
|
|||
|
Mailing Address (if different than above) |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
Zip Code |
City of Birth |
|
|
|
|
|
|
|
|
||
|
Home Phone No |
|
Work Phone No |
Fax No |
Email Address |
|||
|
|
|
|
|
|
|
|
|
Section 2: Optional Enrollment Information
(Completing the information below is optional. It is collected in an effort to track our success in being inclusive of all populations)
Check below what racial/ethnic background best describes you. If you do not identify with any of the choices given, please check the OTHER box and list your preferred choice.
American Indian/Alaskan Native |
Black or African American |
Asian |
Hispanic/Latino/Spanish |
Other: (please list) ___________________________________
Native Hawaiian or other Pacific Islander White
1.What is your primary language?
________________________________________________________________________________________
2. Do you speak any other language(s) in addition to your primary language? |
Yes |
No |
If yes, please list any other language(s) that you speak fluently: |
|
|
________________________________________________________________________________________
3.What language do you speak most often with the children that you work or volunteer with?
________________________________________________________________________________________
Section 3: Workforce Information
What is your Position(s)? |
|
|
|
Administrative Support |
Director |
Teacher |
|
Aide 1 |
Driver |
Nanny |
Teacher’s Aide |
Aide 2 |
Executive Director |
Operator |
Volunteer |
Assistant 1 |
Education Coordinator |
Provider |
Other: (please list) |
Assistant 2 |
Head Teacher |
Substitute Provider |
|
Consultant |
Health/Mental Health Worker |
|
|
Cook |
Manager |
|
|
Level of Education |
|
|
|
Less than High School Diploma |
High School Diploma |
General Educational Development (GED) |
|
Certificate from college, school, or professional association in: ____________________________________________
Master’s degree- MA/MS/MED or other in: ____________________________________________________________
PhD, EdD or other doctoral degree in: ________________________________________________________________
Other (please list degree and field of study): _________________________________________________________________
Continued on back (signature required)
July 2014
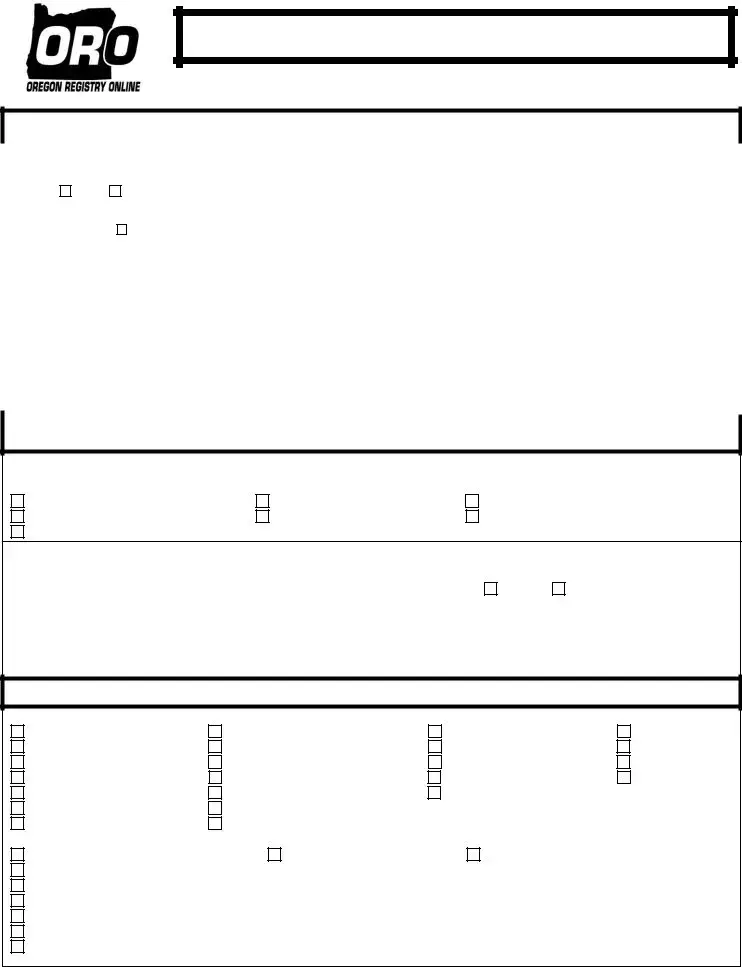
Section 4: Employment/Volunteer Information
Check below what best describes the facility you work or volunteer for:
Child Care Resource & Referral College or University
EI/ECSE
Head Start and/or OPK Health or Mental Health Healthy Start ODE/CACFP Sponsor
Child Care Center/Preschool
Relief Nursery
School District- Elementary or High School Education Family Child Care Provider
State of Oregon Child Care Division
Other: (please list) ______________________________
Name of Facility (list business name. If family child care, list provider’s name)
Facility Phone No
Facility Physical Address (street address, apt no, city, state, zip)
Fax No
Mailing Address (if different than above)
County
Section 5: Childcare Facility Information (Complete this section if you work/volunteer with children)
1. |
Is the facility that you volunteer or work for licensed by the Child Care Division? |
||
|
Yes |
No/Exempt |
Don’t know |
2. |
If yes, check the type of licensed child care facility you are associated with: |
||
Registered Family Child Care Home (RF) |
Certified Family Child Care Home (CF) |
3.If known, please list the facility’s license number: _____________________
Certified Child Care Center (CC)
4. Check below what best describes your work setting:
Child care center |
Child’s own home |
Provider’s home |
Other: (please list) _____________________________________________________
5. Check below the maximum number of hours per day a child may attend the facility:
Four hours or less
More than four hours
6. Check below the maximum number of months in a year that a child may attend the facility:
7. What age groups of children do you work with (check all that apply)?
Infant
Toddler
Preschool
None of the above
Section 6: Enrollment Authorization
Oregon Registry Online (ORO) is a system that will manage your training and education records for licensing requirements and personal professional development. ORO representatives will undertake all necessary precautions to ensure that only authorized personnel will be able to access confidential information. Confidential information will not be disclosed for any purposes other than described here and as authorized by law. By your signature, you consent to the disclosure of your individual contact and training/education information to authorized personnel with the Oregon Office of Child Care, Oregon Center for Career Development, Department of Human Services, and/or the Central coordination of Child Care Resource and Referral at the Teaching Research institute and local child care resource and referral programs.
______________________________ |
___________________________________ |
_____________________ |
Applicant’s Signature |
Printed Name |
Date Signed |
|
|
July 2014 |
Filling out the Oregon Registry Enrollment form is an important step for those involved in childhood care and education. Here are some key takeaways to help you navigate the process effectively:
Completing this form accurately will help streamline your professional journey in child care and education. Take your time, and don’t hesitate to ask for help if needed!
Custody Vs Guardianship - Timely filing of the report is essential to maintain compliance with the court's requirements.
When navigating the sale or purchase of an ATV, having the proper documentation is vital. This ensures a smooth transaction and protects both parties involved. For a thorough understanding of the requirements, explore this essential guide on the ATV Bill of Sale form that outlines everything you need to know.
How Much Does a Divorce Cost in Oregon - Notarization or court clerk signature may be required for some forms included in the packet.
| Fact Name | Fact Description |
|---|---|
| Purpose of the Form | The Oregon Registry Enrollment form is designed to enroll individuals in the Oregon Registry Online system, which tracks professional development in childhood care and education. |
| Governing Law | This form is governed by Oregon Administrative Rules (OAR) related to child care and education. |
| Sections Included | The form consists of several sections, including Individual Information, Optional Enrollment Information, Workforce Information, Employment/Volunteer Information, Childcare Facility Information, and Enrollment Authorization. |
| Confidentiality Assurance | Confidential information collected through this form will only be accessed by authorized personnel and will not be disclosed for any other purposes. |
| Optional Information | Some sections of the form are optional, allowing individuals to provide demographic information to help track inclusivity. |
| Address Updates | Individuals can request the Child Care Division to update their address on file for the Central Background Registry. |
| Professional Roles | The form allows individuals to specify their role in the child care field, such as teacher, director, or volunteer. |
| Education Levels | Applicants can indicate their highest level of education, ranging from less than a high school diploma to a doctoral degree. |
| Childcare Facility Licensing | The form includes questions about whether the facility where the individual works or volunteers is licensed by the Child Care Division. |
| Signature Requirement | A signature is required on the form, indicating consent for the disclosure of contact and training information to authorized entities. |
The Oregon Registry Enrollment form is a crucial document for individuals involved in childhood care and education in Oregon. Along with this form, several other documents are often required to ensure a comprehensive registration process. Here’s a list of those documents with brief descriptions.
These documents collectively support the enrollment process and help maintain high standards in childhood care and education. Ensuring you have all necessary forms completed and submitted will facilitate a smoother registration experience.